
{kind=link}
With necessary Different Cost Mannequin Efficiency Pathway (APP) Reporting starting in Efficiency 12 months 2025, the time to behave is now. Reporting high quality on all beneficiaries marks a significant shift, requiring considerate preparation and strategic planning. In case your Accountable Care Group (ACO) hasn’t began but, don’t fear — there’s nonetheless time to get on monitor.
The primary important step: finalize your plan by figuring out your optimum reporting methodology.
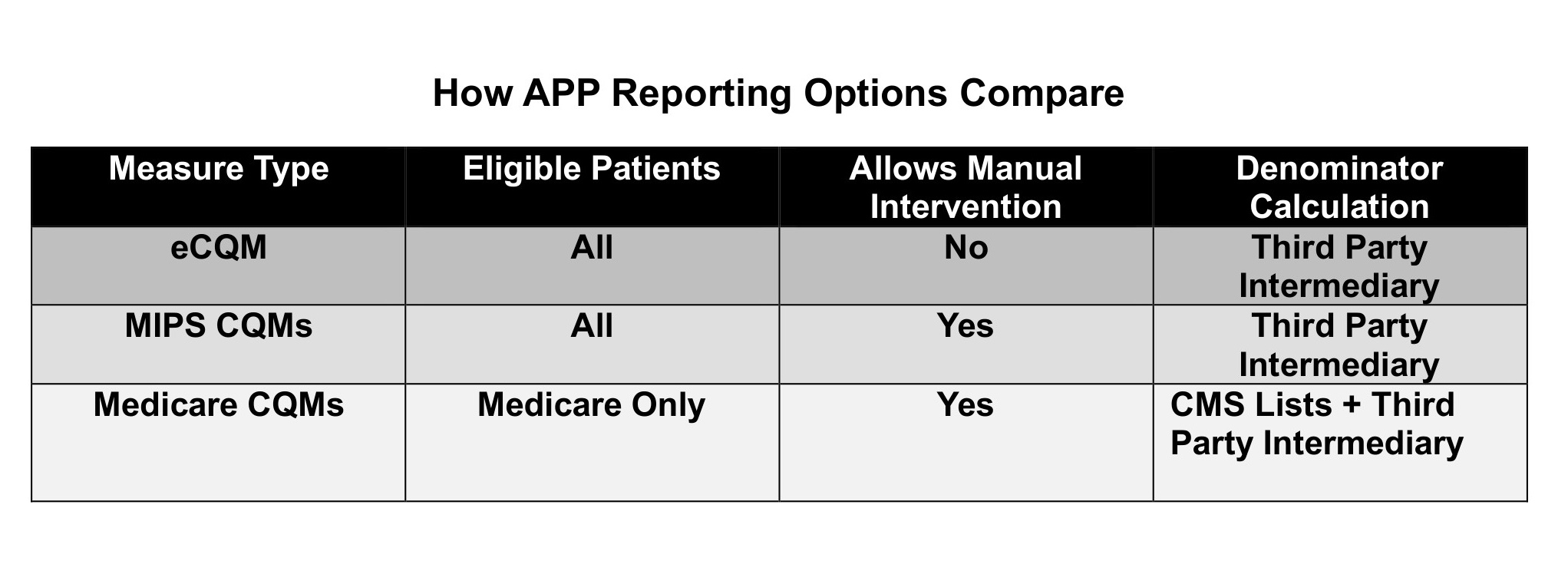
Unsure of the very best methodology to your ACO to carry out APP Reporting? You have got three reporting choices — Digital Medical High quality Measures (eCQMs), Advantage-based Incentive Cost System Medical High quality Measures (MIPS CQMs), and Medicare Medical High quality Measures (Medicare CQMs). Listed here are the variations between these approaches, and why the choice concerning “finest methodology” will not be automated. It should rely in your collaborating doctor practices, their Digital Well being Information (EHRs), and your want for knowledge.
How APP Reporting Choices Evaluate
Understanding whether or not you might have the flexibility to carry out eCQM Reporting is an important first technique.
Why? Many organizations need to use this method as a result of one digital supply doc, a QRDA-I, captures each denominator and numerator of measures. In case your system can do it, it’s straightforward for the group (however most likely the most costly methodology). In the event you can’t meet the circumstances, you have to to carry out APP Reporting by means of both MIPS CQMs or Medicare CQMs. Let’s study the eCQM query first, as a result of it’s the most simple.
eCQMs: Points for APP reporting
eCQMs have plenty of points in APP Reporting as a result of they require a standardized knowledge supply, known as the QRDA-I, which licensed EHRs use as a high quality reporting software to seize and report measures. To make use of eCQMs in APP Reporting, that you must meet two circumstances which can be challenges for multi-EHR ACOs:
- Every particular person follow EHR should be capable of generate a QRDA-I, the info format required for eCQM reporting. You probably have practices with techniques that aren’t ONC-Licensed, or if even one follow has no EHR, you will be unable to satisfy this situation. Even some licensed EHRs should not capable of export a QRDA-I outdoors the system. To make sure that you would be able to meet this situation, you have to to check every follow EHR to validate that you would be able to produce affected person knowledge in a QRDA-I from each follow.
- Affected person knowledge from QRDA-I information throughout all techniques should be aggregated and sufferers should be de-duplicated by means of affected person matching and integration of knowledge. APP Reporting requires that sufferers are uniquely reported solely as soon as, with the newest measure worth. This may require technical work out of your Certified Registry vendor, in case you have multiple EHR.
Are there comparable circumstances for MIPS or Medicare CQMs? Not precisely. CQMs might be reported utilizing any form of knowledge format that may be validated by the affected person’s medical report. However every has benefits and drawbacks.
MIPS CQMs: Increased flexibility, doubtlessly greater value and reporting burden
MIPS CQMs was a most well-liked selection of many ACOs, particularly these with many techniques, due to flexibility in knowledge supply codecs for each numerators and denominators. Your ACO can mixture QRDA-Is, flat information, and any exterior knowledge to make use of in APP Reporting, so long as it’s backed by the medical report. That knowledge is of excessive worth for a lot of different ACO functions, similar to inhabitants well being, value administration, analytics, and well being fairness. EHRs should be capable of produce stories from their techniques, which most can do. This may initially contain ACO or follow employees to generate knowledge information, and require intermittent involvement thereafter.
Medicare CQMs: Information aggregation nonetheless required, highest reporting burden for many ACOs
The Medicare CQM possibility is predicated on the need to restrict ACO workload in knowledge aggregation. However the Facilities for Medicare & Medicaid Providers (CMS) has modified its steering right here. Whereas CMS will likely be offering quarterly lists of sufferers who’re eligible for measures primarily based on claims, these aren’t sufficient. ACOs should validate eligibility with their very own knowledge, which implies that ACOs will nonetheless must mixture knowledge from follow administration techniques to confirm affected person protection, visits, and diagnoses.
Like MIPS CQMs, Medicare CQMs have extra versatile knowledge sources for gathering medical (numerator) knowledge. However for ACOs looking for to decrease their prices and relying on manually trying up and submitting values, this reporting methodology comes with a a lot greater employees burden.
Your choice standards
Your ACO ought to examine which methodology will create probably the most correct, full reporting involving the least work to your group. In case you are a big group with one or two huge techniques, you’ll more than likely be capable of produce QRDA-Is or FHIR information to satisfy the necessities. In case you are a smaller group with a number of techniques, that you must take a look at your follow techniques’ outcomes first.
In case your ACO has been struggling to determine which methodology is “superior” for APP Reporting, we will guarantee you that any of those strategies can produce true and correct outcomes. Which is perfect, alternatively, will rely in your ACO limits and targets:
- If value is your greatest concern, use Medicare CQMs — however perceive that, relying in your affected person rely, it would require employees work. Because the variety of measures grows, so will the work.
- In case your long-range aim is driving outcomes and well being fairness, your answer will finally want extra knowledge. You can begin with Medicare CQMs, however plan to make use of eCQMs or MIPS CQMs for the next yr.
Do not forget that the final word CMS plan is to require extra measures and (interoperable) digital measures, which is able to construct towards a extra sturdy knowledge answer sooner or later. Taking steps now’s the easiest way to get began for long-term reporting options.
Picture: Witthaya Prasongsin, Getty Photographs

Theresa (Terry) Hush is a well being care strategist and alter skilled with expertise throughout the well being care spectrum. Terry’s broad vary of well being care expertise contains government positions in public, non-profit and personal sectors, from each payer and supplier sides of the enterprise, peppered with well being care public coverage and regulation expertise. She is co-founder and CEO of Roji Well being Intelligence, fashioned in 2002 to assist suppliers implement Worth-Primarily based Care with know-how and data-guided providers. An skilled at creating consensus for desired change by means of schooling and collaboration, Terry helps organizations to maneuver towards value and final result accountability to realize development.
This submit seems by means of the MedCity Influencers program. Anybody can publish their perspective on enterprise and innovation in healthcare on MedCity Information by means of MedCity Influencers. Click on right here to learn the way.